
 Sample Submission Guidelines
Sample Submission Guidelines
Comparative Overview of cfDNA and ctDNA: Biology, Utility, and Extraction
Cell-free DNA (cfDNA) and circulating tumor DNA (ctDNA) are both valuable biomarkers in liquid biopsies, but they differ in origin, biological significance, and clinical applications. Understanding these differences is crucial for selecting the right extraction and analysis methods for diagnostic, prognostic, and monitoring purposes. This guide explains their biological differences, optimal extraction methods, and real-world applications-with practical tips for researchers and clinicians.
1. Fundamental Differences Between cfDNA and ctDNA
cfDNA and ctDNA exhibit distinct biological origins and molecular profiles. cfDNA primarily originates from apoptotic or necrotic normal cells, displaying a characteristic peak at 166 bp due to nucleosomal protection. In healthy individuals, its plasma concentration ranges from 1-100 ng/mL, and it typically carries no somatic mutations. These features make cfDNA an excellent biomarker for monitoring general cellular turnover and systemic physiological states.
In contrast, ctDNA is specifically released by tumor cells through necrosis, apoptosis, or active secretion. It exhibits a bimodal size distribution, including short fragments (<150 bp) and longer DNA strands. Although ctDNA usually constitutes <1% of total cfDNA, its tumor-specific mutations (e.g., in EGFR or TP53) enable highly specific liquid biopsy applications for cancer detection.
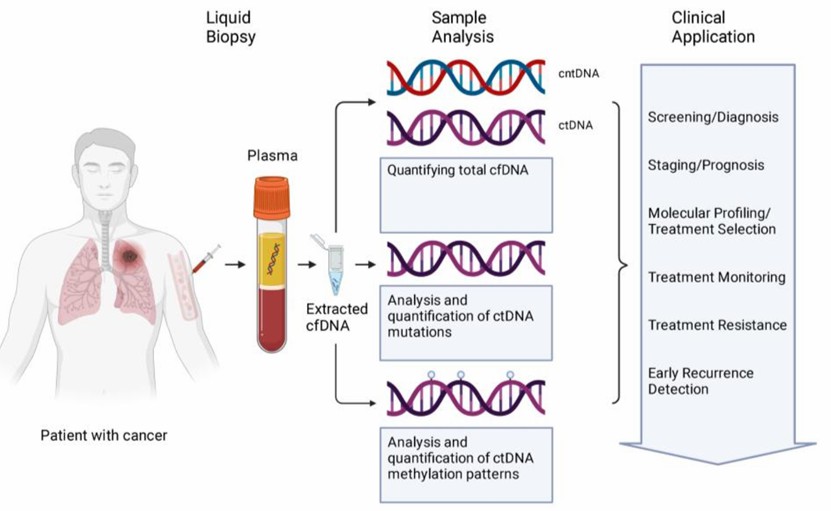 Figure 1. cfDNA from liquid biopsy samples are analyzed in several ways.( Jonathan Dao, et. al,2023)
Figure 1. cfDNA from liquid biopsy samples are analyzed in several ways.( Jonathan Dao, et. al,2023)
| Feature | cfDNA | ctDNA |
|---|---|---|
| Source | Apoptotic/necrotic normal cells | Tumor cells (via necrosis, apoptosis, or secretion) |
| Fragment Size | Predominantly 166 bp (nucleosomal) | Shorter (<150 bp) + longer fragments |
| Concentration | 1-100 ng/mL plasma (healthy) | Often <1% of total cfDNA |
| Mutations | Wild-type | Tumor-specific (e.g., EGFR, TP53) |
- cfDNA reflects general cellular turnover.
- ctDNA carries cancer-specific alterations, enabling liquid biopsies.
2. Extraction Methods: Tailoring to Your Needs
The choice of extraction method for cfDNA and ctDNA depends on sample type, downstream applications, and target fragment size. Pre-analytical handling is critical to ensure high-quality yields, particularly for rare ctDNA variants.
2.1 Pre-Analytical Considerations
- Blood Collection:
cfDNA: EDTA tubes (process within 2-4 hours).
ctDNA: Streck tubes (stable for 7 days at room temperature).
- Plasma Prep: Double-centrifuge (1,600 × g → 16,000 × g) to remove cells.
2.2 Comparison of Extraction Techniques
| Method | Best for cfDNA? | Best for ctDNA? | Why? |
|---|---|---|---|
| Silica Columns | ✅(QIAamp CNA Kit) | ❌ (loses short fragments) | High purity but misses small ctDNA |
| Magnetic Beads | ✅(Good recovery) | ✅ (MagMAX, Dynabeads) | Better recovery of <150 bp fragments |
| Phenol-Chloroform | ❌ (low yield) | ❌ (high background) | Outdated for low-abundance targets |
Pro Tip: For ctDNA, add carrier RNA to improve recovery of rare fragments.
Services you may interested in
Learn More
3. Detection & Analysis: Sensitivity Matters
The choice of detection methods for cfDNA and ctDNA must account for their distinct biological and clinical requirements. CfDNA analysis typically employs qPCR (ALU repeats) for quantification due to its cost-effectiveness and reliability in measuring total circulating DNA. In contrast, ctDNA demands ultra-sensitive techniques like ddPCR to detect rare tumor-derived mutations at frequencies as low as 0.01%.
For comprehensive profiling, whole-genome/exome sequencing (WGS/WES) provides broad coverage of cfDNA, making it suitable for non-cancer applications (e.g., NIPT, transplant monitoring). However, targeted NGS panels (e.g., Guardant360) are preferred for ctDNA, as they enhance sensitivity for cancer-specific variants while reducing costs.
Size analysis further differentiates the two:
cfDNA: Standard Bioanalyzer assessment confirms the expected ~166 bp nucleosomal pattern.
ctDNA: Fragmentomics (DELFI score) leverages aberrant fragmentation profiles to improve tumor detection, particularly in early-stage disease.
| Application | cfDNA Tools | ctDNA Tools |
|---|---|---|
| Quantification | qPCR (ALU repeats) | ddPCR (for rare mutations) |
| Profiling | WGS/WES | Targeted NGS panels (e.g., Guardant360) |
| Size Analysis | Bioanalyzer | Fragmentomics (DELFI score) |
Case Study: Non-Invasive Early-Stage Lung Cancer Diagnosis via ctDNA Methylation Profiling (Liang et al., 2019)
Targeted DNA methylation sequencing of ctDNA could effectively diagnose early-stage lung cancer, achieving 92.7% sensitivity and 92.8% specificity in tissue analysis of 230 pulmonary nodules (<3cm). When applied to plasma samples, the optimized 9-marker panel maintained 79.5% sensitivity (85.7% for stage IB) and 85.2% specificity in distinguishing malignant from benign lesions, while showing 93.2% specificity in 118 healthy controls. Notably, the assay detected 75% of stage IA cancers, addressing a critical need in early diagnosis, and demonstrated the potential to reduce unnecessary biopsies by 85% in benign cases, significantly outperforming LDCT screening in false-positive reduction. These findings established ctDNA methylation analysis as a promising non-invasive approach for early lung cancer detection and pulmonary nodule triage.
Significance: First demonstration that ctDNA methylation sequencing enables non-invasive early lung cancer diagnosis, establishing important groundwork for liquid biopsy development.
4. Clinical Applications: Where Each Shines
The distinct biological properties of cfDNA and circulating tumor ctDNA determine their unique clinical utilities. While cfDNA is derived from normal cell turnover and can originate from various tissues, ctDNA is specifically shed by tumor cells, carrying cancer-associated mutations and epigenetic alterations. This fundamental difference dictates their applications in non-cancer diagnostics versus oncology.
4.1 Non-Cancer Uses of cfDNA
cfDNA has emerged as a powerful tool in non-oncological diagnostics due to its minimally invasive nature and broad tissue representation. Key applications include:
1) Non-Invasive Prenatal Testing (NIPT)
Fetal Aneuploidy Detection: cfDNA from placental origin (also called cell-free fetal DNA, cffDNA) enables highly accurate screening for chromosomal abnormalities such as Trisomy 21 (Down Syndrome), Trisomy 18 (Edwards Syndrome), and Trisomy 13 (Patau Syndrome).
Performance: For Trisomy 21 (T21), NIPT achieves >99% sensitivity and specificity, significantly reducing the need for invasive procedures like amniocentesis.
Expanding Applications: Recent advances allow detection of microdeletions, fetal sex determination, and single-gene disorders through targeted sequencing.
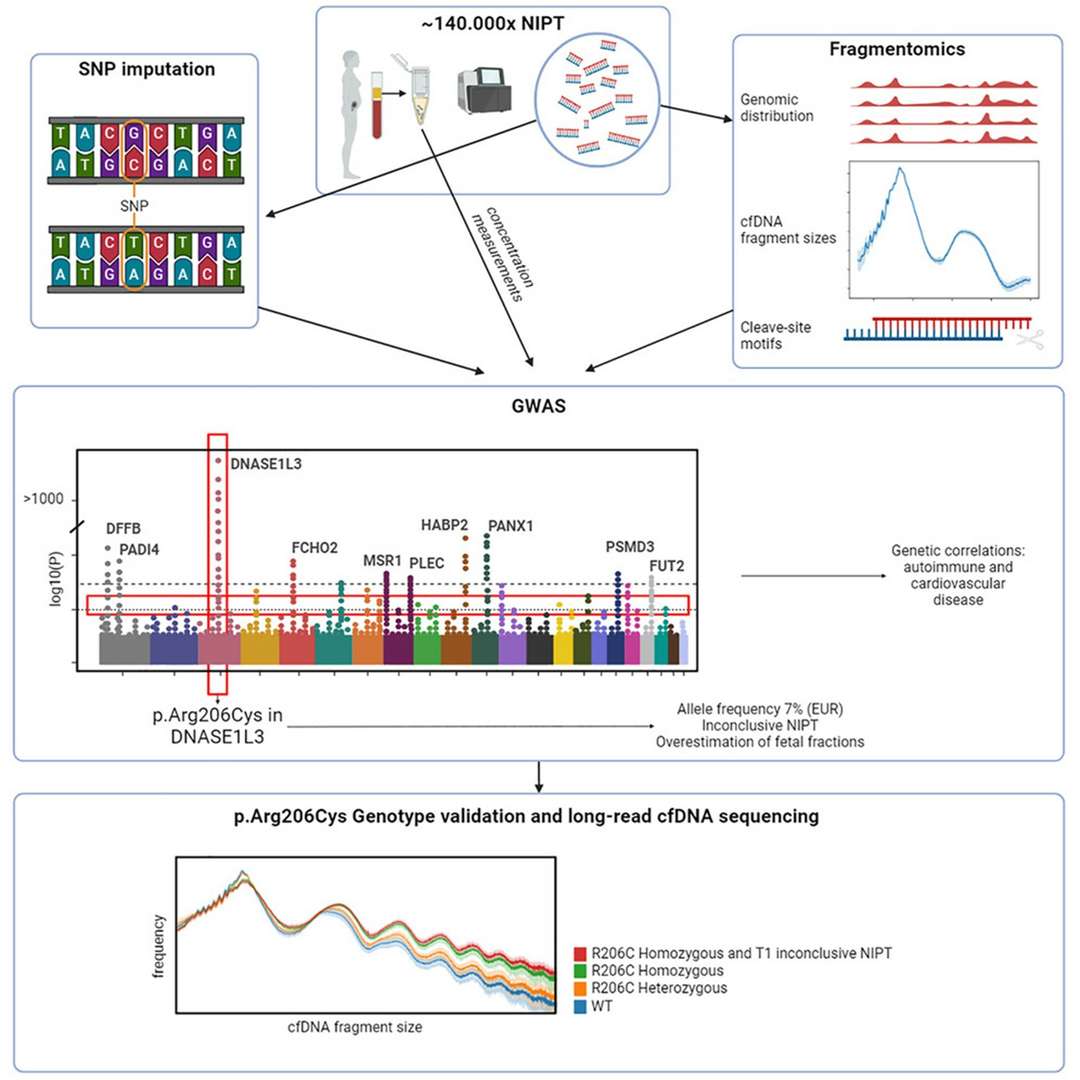 Figure 2.Common genetic variants and cfDNA characteristics.( Jasper Linthorst, et. al,2024)
Figure 2.Common genetic variants and cfDNA characteristics.( Jasper Linthorst, et. al,2024)
2) Transplant Rejection Monitoring
Donor-Derived cfDNA (dd-cfDNA): After organ transplantation, elevated levels of donor-derived cfDNA in the recipient's blood correlate with allograft injury or rejection.
Diagnostic Accuracy: Studies report an AUC (Area Under the Curve) of 0.91, making it a reliable biomarker for early rejection detection, particularly in heart and kidney transplants.
Advantages Over Biopsy: Unlike invasive tissue biopsies, dd-cfDNA offers a real-time, dynamic assessment of graft health, enabling timely intervention.
3) Other Emerging Applications
Autoimmune Diseases: cfDNA methylation patterns may help monitor disease activity in lupus (SLE) and rheumatoid arthritis.
Sepsis & Trauma: Elevated cfDNA levels correlate with tissue damage severity, aiding in prognosis and therapeutic response assessment.
4.2 Oncology Applications of ctDNA
ctDNA, carrying tumor-specific mutations, has revolutionized liquid biopsy in cancer management. Its applications span:
1) Early Detection & Screening
Multi-Cancer Early Detection (MCED): Panels targeting methylation patterns and somatic mutations can identify multiple cancer types (e.g., lung, breast, colorectal) at early stages.
High-Risk Populations: Useful for Lynch syndrome, BRCA carriers, and heavy smokers to detect malignancies before clinical symptoms arise.
2) Treatment Selection & Personalized Therapy
Identifying Targetable Mutations: ctDNA analysis detects EGFR, KRAS, BRAF, and PIK3CA mutations, guiding tyrosine kinase inhibitor (TKI) or immunotherapy choices.
Resistance Monitoring: Emergence of EGFR T790M or ALK resistance mutations in NSCLC can prompt therapy adjustments.
3) Minimal Residual Disease (MRD) & Recurrence Monitoring
Post-Surgical Surveillance: ctDNA positivity after tumor resection predicts relapse months before imaging (e.g., in colorectal and breast cancers).
Dynamic Risk Stratification: Serial ctDNA tracking helps distinguish patients needing adjuvant therapy from those with low recurrence risk.
4) Therapeutic Response Assessment
Real-Time Efficacy Monitoring: Declining ctDNA levels post-treatment correlate with tumor regression, while rising levels indicate progression or resistance.
Clinical Trials: ctDNA is increasingly used as a surrogate endpoint in trials to accelerate drug development.
| Use Case | Example |
|---|---|
| Early Detection | GRAIL's Galleri test (50+ cancers) |
| Treatment Monitoring | EGFR T790M in NSCLC (Guardant360 CDx) |
| MRD Detection | Signatera (tumor-informed assays) |
Real-World Impact:
The BESPOKE-CRC trial demonstrated ctDNA's clinical utility, where ctDNA-guided therapy reduced unnecessary chemotherapy by 48% in colorectal cancer patients, avoiding overtreatment while maintaining efficacy.
5. Troubleshooting Guide
Effective cfDNA/ctDNA analysis requires addressing three major challenges: low yield, gDNA contamination, and PCR inhibition. For low yields, increasing plasma volume (≥4 mL) boosts cfDNA recovery, while bead-based extraction optimizes ctDNA capture of rare fragments. To combat gDNA contamination, DNase treatment works well for cfDNA, whereas ctDNA benefits from double centrifugation (1,600g → 16,000g) combined with size selection. For PCR inhibition, simple dilution (1:5) often suffices for cfDNA, but ctDNA analysis requires dedicated inhibitor removal steps due to its ultra-low abundance. A critical pre-analytical consideration is hemolysis-indicated by pink plasma discoloration-which increases wild-type DNA and masks ctDNA signals. Preventive measures include using blunt needles during blood collection, implementing spectrophotometric QC (A414/A375 ratios), and incorporating spike-in controls for extraction validation. By applying these targeted solutions, researchers can significantly improve detection sensitivity for both cfDNA (general biomarkers) and ctDNA (tumor-specific signals), ensuring reliable results across diverse applications from cancer monitoring to non-invasive prenatal testing.
Common Challenges
| Issue | cfDNA Solution | ctDNA Solution |
|---|---|---|
| Low Yield | Increase plasma volume (≥4 mL) | Use bead-based extraction |
| gDNA Contamination | DNase treatment post-extraction | Double-centrifuge + size selection |
| PCR Inhibition | Dilute sample 1:5 | Add inhibitor removal step |
Critical Note: Hemolysis increases wild-type DNA, masking ctDNA signals-always check plasma for pink discoloration!
6. Conclusion
The comprehensive comparative analysis of cfDNA and ctDNA elucidates their distinct yet complementary roles in advancing modern diagnostic paradigms and therapeutic monitoring strategies. These circulating nucleic acids offer unique windows into human health and disease states as two critical components of liquid biopsy technologies. cfDNA, with its broad representation of cellular turnover dynamics, serves as a powerful systemic biomarker, providing indispensable clinical utility in three key areas: (1) NIPT, where it has revolutionized fetal genetic screening with >99% detection rates for common trisomies; (2) solid organ transplant surveillance, enabling sensitive detection of graft rejection through donor-derived DNA quantification; and (3) inflammatory disease monitoring, offering real-time assessment of disease activity in conditions like lupus and rheumatoid arthritis.
Conversely, ctDNA has emerged as a transformative tool in oncology, with three principal clinical applications demonstrating its unique value: (1) early cancer detection, particularly for hard-to-diagnose malignancies like pancreatic and ovarian cancers, where recent studies (e.g., DETECT-A trial) have shown detection rates exceeding 70% for stage I/II disease; (2) therapy selection, where ctDNA profiling identifies actionable mutations with 90-95% concordance with tissue biopsies (as demonstrated in the TARGET trial); and (3) minimal residual disease monitoring, with tumor-informed ctDNA assays predicting recurrence 6-9 months before radiographic evidence (per TRACERx data).
The integration of these analytes in clinical practice requires careful consideration of their distinct biological characteristics. While cfDNA analysis benefits from standardized isolation protocols and relatively abundant yields (typically 5-100 ng/mL plasma), ctDNA detection demands ultra-sensitive approaches due to its low fractional abundance (<0.1% in early-stage cancers). Emerging solutions to these challenges include: (1) novel preservation tubes (e.g., Streck cfDNA BCT) that maintain sample integrity, (2) optimized extraction methods favoring magnetic beads over columns for short-fragment recovery, and (3) advanced detection platforms combining ultra-deep sequencing (100,000× coverage) with error-correction algorithms.
Future directions in the field point toward three transformative developments: (1) multi-analyte liquid biopsy panels integrating cfDNA, ctDNA, methylation, and fragmentomics signatures; (2) point-of-care microfluidic platforms enabling rapid turnaround; and (3) artificial intelligence-driven interpretation algorithms. As these technologies mature, they promise to establish liquid biopsy as a cornerstone of precision medicine, with projected market growth to $28 billion by 2028 according to recent industry analyses.
For optimal clinical implementation, we recommend: (1) adopting consensus pre-analytical standards (e.g., CLSI guidelines) to minimize variability, (2) validating assay performance in intended-use populations, and (3) developing interdisciplinary workflows combining laboratory medicine, bioinformatics, and clinical expertise. By strategically leveraging the complementary strengths of cfDNA and ctDNA, the medical community can realize the full potential of liquid biopsies to transform disease detection, monitoring, and management across diverse clinical contexts.
References:
- Dao, J., Conway, et, al., (2023). Using cfDNA and ctDNA as Oncologic Markers: A Path to Clinical Validation. International journal of molecular sciences, 24(17), 13219. https://doi.org/10.3390/ijms241713219
- Liang, W., Zhao, Y., et.al., (2019). Non-invasive diagnosis of early-stage lung cancer using high-throughput targeted DNA methylation sequencing of circulating tumor DNA (ctDNA). Theranostics, 9(7), 2056-2070. https://doi.org/10.7150/thno.28119
- Linthorst, J., Nivard, M., & Sistermans, E. A. (2024). GWAS shows the genetics behind cell-free DNA and highlights the importance of p.Arg206Cys in DNASE1L3 for non-invasive testing. Cell reports, 43(10), 114799. https://doi.org/10.1016/j.celrep.2024.114799


